
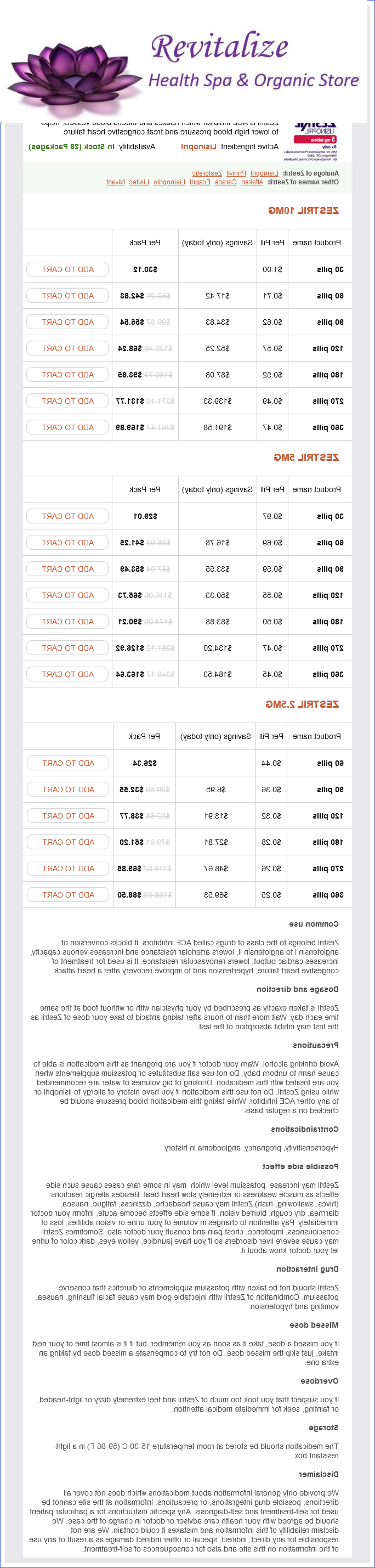
Zestril dosages: 10 mg, 5 mg, 2.5 mg
Zestril packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
Only $0.26 per item
In stock: 931
Description
An acute ulcer is simply an extension of an erosion through the full thickness of the mucosa in to the submucosa or deeper in to underlying tissues arteria aorta definicion buy zestril 5 mg online. They tend to be larger than erosions and frequently occur in areas of intense erosion and mucosal congestion hypertension 2013 guidelines zestril 2.5 mg overnight delivery, especially on the greater curvature of the stomach. The ulcer bed is similar to that of an erosion and fibrous scar tissue is not prominent in the base. Acute ulcers are considerably less common in the duodenum but in that site they tend to be single. Haemorrhage is a frequent complication of acute ulcer due to ulceration of submucosal vessel walls. Chronic peptic ulcers, by contrast, are long standing, by definition, and characterised histologically by loss of the full thickness of the mucosa with a variable degree of penetration in to the underlying coats and the presence of fibrous tissue in the ulcer base. An ulcer may be regarded as chronic, clinically, when it has failed to heal over a 122 Stomach reasonable period of time and, pathologically, when attempts at repair have led to the formation of collagenous fibrohyaline basal scar to such a degree that restoration of the submucosa and muscularis propria is no longer possible; there is often concomitant failure of the mucosa to regenerate satisfactorily. It is generally assumed that all chronic ulcers originate in an acute ulcer that failed to heal. The overlying serosa is often thickened and opaque, and the ulcer base adheres to underlying or overlying strictures, particularly the pancreas. The presence of gastritis, either local or more generalised, can be confirmed on microscopy. Lesser curve ulcers tend to enlarge in a saddle-shaped manner and may reach 100 mm or more in diameter [145]. Many arise at the junction of antral and corpus mucosa surrounded by pyloric-type mucosa or metaplastic mucosa of intestinal type, whereas others arise entirely in antral mucosa [147,149]. They are usually single, although multiple ulcers can occur in 613% of cases [147,150]. They occur predominantly on the lesser curvature and less often on the posterior wall. The edges are clear cut but not raised or rolled and overhang, producing a flasklike appearance. The base is grey and either blood clot or an eroded vessel can occasionally be seen within the crater. All large ulcers have to be distinguished from carcinomas and examined closely; distinction can usually be made by the clear-cut overhanging edges and absence of thickening in adjacent mucosa, but multiple biopsies should be taken from the base and circumference to exclude malignancy. Microscopic pathology of peptic ulcers Erosions show necrosis of a small area of mucosa of variable depth but not extending down to the muscularis mucosae. The crater of the erosion contains necrotic slough, polymorphs and red blood cells. There is a variable, usually minor, degree of acute inflammation in the adjacent lamina propria with dilatation and congestion of nearby capillar- ies. On healing most erosions show complete mucosal regeneration and there is no visible residual scarring. Then there is a zone of granulation tissue of variable vascularity containing young fibroblasts and mononuclear inflammatory cells.
Syndromes
- Name of product (ingredients and strength, if known)
- If the stroke is caused by a blood clot, a clot-busting drug may be given to dissolve the clot.
- Nutritionists and dieticians
- Wear sunglasses that screen ultraviolet light when you are exposed to sunlight, even during the winter.
- Is the pain constant or does it come and go? Has the pain become more severe?
- Coma
Toxicological cardiomyopathy is often manifested in the form of eccentric hypertrophy pulse pressure 30 mmhg zestril 5 mg purchase free shipping. The development of cardiac hypertrophy can be divided in to three stages: developing hypertrophy blood pressure which arm zestril 2.5 mg without a prescription, during which period the cardiac workload exceeds cardiac output; compensatory hypertrophy, in which the workload/mass ratio is normalized and normal cardiac output is maintained; decompensatory hypertrophy, in which ventricular dilation develops and cardiac output progressively declines, and overt heart failure occurs (Richey and Brown, 1998). However, it is difficult to apply this knowledge to patients: first, acquired cardiac disease such as heart failure is the result of interaction between environmental factors and genetic susceptibility, indicating the role of polymorphisms. Second, extrinsic and intrinsic stresses produce lesions that cannot be explained by a single gene or a single pathway, suggesting complexity between deleterious factors and the heart. Cardiac toxicity is the critical link between environmental factors and myocardial pathogenesis. For a better understanding of cardiac toxicology, a triangle model of cardiac toxicity is presented in. In this model, complexity of the interaction between environmental stresses and the heart, and the balance between myocardial protection and deleterious dose and time effects are considered. First, it is important to recognize that chemicals can lead to heart failure without heart hypertrophy. Second, a chemical can lead to activation of both protective and destructive responses in the myocardium. Third, long-term toxicological responses often result in maladaptive hypertrophy, which primes the heart for malignant arrhythmia, leading to sudden cardiac death or transition to heart failure. In the study of cardiac toxicology, the manifestations of cardiac toxicity in human patients and animal models are critical parameters serving as indices of cardiac toxicity. These manifestations are expressed in the forms of cardiac arrhythmia, hypertrophy, and heart failure. These abnormal changes reflect myocardial functional alterations resulting from both acute and chronic cardiac toxicity. Although some changes including cardiac hypertrophy were viewed as a compensatory response to hemodynamic changes in the past, more recent studies suggest that cardiac hypertrophy is a maladaptive process of the heart in response to intrinsic and extrinsic stresses (van Empel and De Windt, 2004; Berenji et al. Cardiac hypertrophy is a risk factor for sudden cardiac death and has a high potential to progress to overt heart failure. Therefore, a distinction between compensatory and maladaptive responses is critical for treatment of patients with toxicological cardiomyopathy. Heart Failure A traditional definition of heart failure is the inability of the heart to maintain cardiac output sufficient to meet the metabolic and oxygen demands of peripheral tissues. This definition has been modified to include changes in systolic and diastolic function that reflect specific alterations in ventricular function and abnormalities in a variety of subcellular processes (Piano et al. Therefore, a detailed analysis to distinguish right ventricular from left ventricular failure can provide a better understanding of the nature of the heart failure and predicting the prognosis.
Specifications/Details
atomic number 53 (Iodine). Zestril.
- Conditions related to too much thyroid gland activity (hyperthyroidism).
- Foot ulcers associated with diabetes.
- Are there safety concerns?
- Dosing considerations for Iodine.
- Radiation emergency associated with the use of radioactive iodides.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96085
Juvenile polyposis syndrome Juvenile polyposis syndrome is an autosomal dominant disorder defined by the presence of five or more juvenile polyps in the colorectum hypertension lifestyle modifications trusted zestril 2.5 mg, juvenile polyps throughout the gastrointestinal tract or any number of juvenile polyps and a positive family history of juvenile polyposis [24 heart attack 6 hours 2.5 mg zestril purchase mastercard,27]. The incidence of juvenile polyposis syndrome is approximately 1/100 000 live births. Typically juvenile polyps are characterised by a prominent lamina propria with oedema and inflammatory cells and cystically dilated glands lined by cuboidal to columnar epithelium with reactive changes. This polyp shows relatively less stroma, fewer dilated glands and more proliferative smaller glands. One is a generalised form that occurs in infancy, in which polyps are present in the stomach, small bowel and colon. These infants have diarrhoea, haemorrhage, malnutrition and intussusception, and death is usual at an early age. In addition, many of these patients have congenital abnormalities, including macrocephaly and generalised hypotonia [5]. The second form, called generalised juvenile polyposis or juvenile polyposis coli, usually presents later in childhood or in adult life and may be sporadic/new or inherited [34]. This form is characterised by the presence of gastrointestinal juvenile polyposis and an increased risk of gastrointestinal cancer [35]. Also, a variety of extra-intestinal manifestations has been reported in about 1078% of these patients [5]. Polyps in juvenile polyposis syndrome predominantly occur in the colorectum, varying in number from five to several hundreds (see Chapter 37). A few studies have examined upper gastrointestinal tract involvement in juvenile polyposis more systematically [3840]. One study found duodenal polyps in 4 of 12 patients with juvenile polyposis syndrome (33%), with two patients having multiple polyps ranging in size from 5 mm to 15 mm and two patients with minute polyps [38]. Other workers have found small intestinal polyps, beyond the range of standard gastroscopy, in 2 of 10 (20%) patients who underwent capsule endoscopy and duodenal polyps in 4 other patients (40%) [40]. Another study reported small bowel polyps in 8 of 56 patients with juvenile polyposis syndrome (14%) [39]. In addition, there are a number of case reports of duodenal, jejunal and ileal polyps in patients with juvenile polyposis syndrome [34,4144]. Moreover, juvenile polyps are frequently found in the ileal pouch of juvenile polyposis patients who have undergone proctocolectomy [45,46]. Histologically, small intestinal polyps in juvenile polyposis syndrome have been classified as juvenile [39,41], hyperplastic and/or inflammatory polyps [38,42,44] and normal mucosa raised by lymphoid hyperplasia [42,43]. In addition, juvenile/hamartomatous polyps with dysplastic changes and adenomas have been found in the duodenum, jejunum and ileum of patients with juvenile polyposis syndrome [38,39,44]. Juvenile polyposis is associated with an increased risk of gastrointestinal cancer. A recent cancer risk analysis calculated a cumulative life-time risk for colorectal cancer in juvenile polyposis syndrome of 39% and a relative risk of colorectal cancer of 34 [47]. However, this may be a conservative estimate because some patients in this study had undergone prophylactic colectomy.
Related Products
Usage: q.d.
Congenital diverticula are often out-pouchings of the full-thickness intestinal wall including muscle coats blood pressure medication news generic zestril 5 mg buy on line. The majority hypertension kidney infection generic 2.5 mg zestril fast delivery, which are of midgut origin, and vary in size from small to the so-called giant diverticula, are not associated with vertebral anomalies. Multiple jejunal diverticula are not uncommon, especially in postmortem examination practice. They are mainly asymptomatic and often discovered only incidentally during investigation for other conditions. They are found incorporated in to the bowel wall, lying on its serosal aspect or in the mesentery, posterior mediastinum or pelvis, detached and separate from the tract. Those cysts that lie within the bowel wall can be submucosal, intramuscular or subserosal in position and may secondarily invaginate in to the lumen, producing symptoms and signs of obstruction, especially in the duodenum or at the ileo-caecal valve. Those that are detached are usually surrounded by smooth muscle and, if they are of foregut origin, may be associated with anomalies of spinal cord and vertebrae. All types of cyst have a mucosal lining of alimentary-type epithelium that may be more primitive than the normal. Rarely cysts, fistulae, sinus tracks or diverticula, lined by alimentary-type epithelium and often surrounded by smooth muscle, are found either beneath the skin that covers the dorsal vertebral spines or opening on to it. There is always an associated vertebral defect, sometimes with local duplication of the spinal cord. It is clear that endoderm giving rise to bowel has failed to separate from ectoderm giving rise to skin and spinal cord, and that mesoderm has failed to grow inward to form normal vertebrae. Cysts containing alimentary epithelium described in the spinal cord are of similar origin [82]. Intussusception, intraluminal obstruction, infarction [83], perforation and haemorrhage have all been described. Causative factors of diverticula and cysts Earlier theories must be discarded, including imperfect luminal recanalisation and the outgrowth of epithelium through the bowel wall [84]. Many diverticula and cysts of foregut and hindgut origin are associated with vertebral anomalies or the KlippelFeil syndrome [70,72,74]; midgut anomalies do not have this association but are otherwise similar. In the 2- to 4-mm embryo, the endoderm, which forms the roof of the yolk sac and is destined to give rise to the future foregut and hindgut, is in contact with the ectoderm, which forms the floor of the amniotic sac and will give rise to the neural crest and tube. This canal normally closes and the notochord grows forward to become intercalated with the endoderm and separate it from the ectoderm. Mesoderm grows inward to surround the notochord and form the future vertebrae and surrounding muscle; this separates the ectoderm and endoderm still further. At the same time the midgut develops from the yolk sac and thus has no relationship to the ectoderm. Failure of separation of ectoderm from endoderm at this early stage would explain the formation of diverticula and cysts of the foregut and hindgut, and their association with spinal cord abnormalities. Failure of mesoderm to grow inwards would explain the vertebral anomalies [85,86] and development of the midgut from the yolk sac, which is unrelated to the ectoderm, provides the reason for the non-association of neural and vertebral anomalies with midgut anomalies. Duodenocolic fistulae Examples of fistulae between the third part of the duodenum and the transverse colon are described which are thought to have developed at the time of physiological herniation [88].
Additional information:
8 of 10
Votes: 282 votes
Total customer reviews: 282
Tags: buy zestril 2.5 mg online, buy generic zestril 2.5 mg on line, generic zestril 2.5 mg buy on line, purchase 10 mg zestril overnight delivery, order 2.5 mg zestril, safe 10 mg zestril, discount 2.5 mg zestril, order zestril 5 mg
Customer Reviews
Connor, 24 years: Studies in rats have shown early changes in the basement membrane of endothelial cells of the capillaries and postcapillary venules, leading to obliteration of small vessels and ischemic infarcts in the large intestine. The main value of a biopsy in infective disease is in those patients who are culture negative [78]. The deep muscle layers can be normal or show varying degrees of disorganisation by granulation tissue and fibrosis. If no germline mutation is found in such an at-risk person, he or she does not have juvenile polyposis syndrome and can be followed in accordance with the guidelines for screening programmes for the general population [52].
Esiel, 53 years: Immunoassay of gastric intrinsic factor and the titration of antibody to intrinsic factor. The cytoplasm, located apically above an oval nucleus, contains eosinophilic apical granules that are easily visualised on H&E. Unlike in PeutzJeghers polyps, dysplasia is frequently found in the polyps of juvenile polyposis syndrome. Inflammatory disorders of the stomach 129 cantly increased in number, sometimes forming small clusters or microcarcinoids [250,251].
Trompok, 51 years: Polymorphonuclear leukocytosis is usually present and pyrexia is common but not invariable. In fact, neurons are the only cell type with such a Nissl substance, reflecting the unusual demand for protein synthesis. Immune aspects of intestinal metaplasia of the stomach: an immunohistochemical study. Myelin formation proceeds by a progressive wrapping of multiple layers of the myelinating cell around the axon, with extrusion of the cytoplasm and extracellular space to bring the lipid bilayers in to close proximity.