
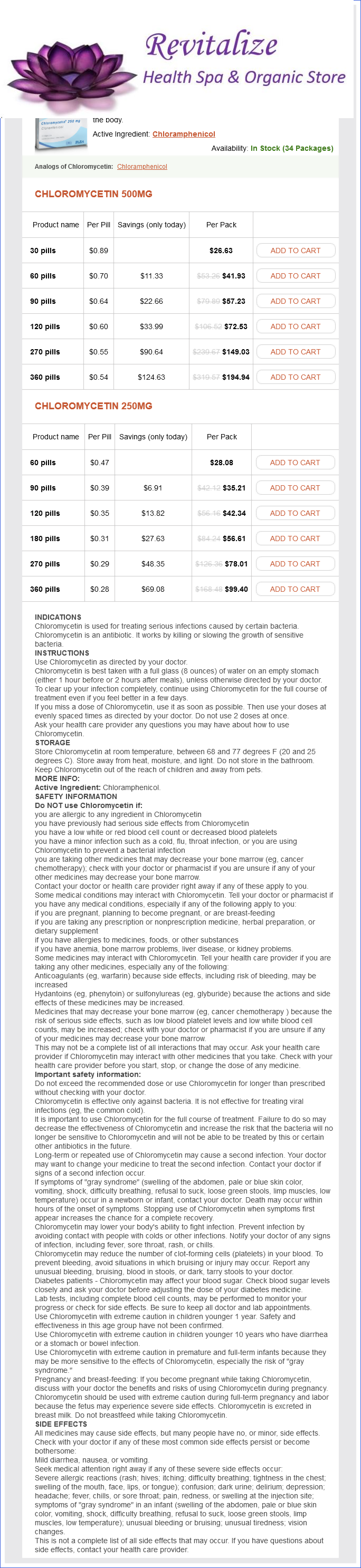
Chloromycetin dosages: 500 mg, 250 mg
Chloromycetin packs: 30 pills, 60 pills, 90 pills, 120 pills, 270 pills, 360 pills, 180 pills
Only $0.29 per item
In stock: 903
Description
Autoimmune adrenalitis results from the destruction of the adrenal cortex by organspecific autoantibodies treatment zinc toxicity 500 mg chloromycetin purchase, with 21-hydroxylase as the common antigen medicine hat jobs chloromycetin 250 mg visa. If the patient is seriously ill or hypotensive, hydrocortisone 100 mg should be given intravenously or intramuscularly together with intravenous 0. Ideally this should be done immediately after a blood sample is taken for later measurement of plasma cortisol. These symptoms may be the prelude to an Addisonian crisis with severe hypotension and dehydration precipitated by intercurrent illness, accident or operation. Pigmentation (dull, slaty, grey-brown) is the predominant sign in over 90% of cases. Postural systolic hypotension, due to hypovolaemia and sodium loss, is present in 8090% of cases, even if supine Table19. Electrolytes and urea classically show hyponatraemia, hyperkalaemia and a high urea, but they can be normal. Chest and abdominal X-rays may show evidence of tuberculosis and/or calcified adrenals. Subsequent requirements are several litres of saline within 24 hours (assessing with central venous pressure line if necessary) plus hydrocortisone, 100 mg i. Oral replacement medication is then started, unless unable to take oral medication, initially hydrocortisone 20 mg, 8-hourly, reducing to 2030 mg in divided doses over a few days (Table 19. Fludrocortisone is unnecessary acutely as the high cortisol doses provide sufficient mineralocorticoid activity it should be introduced later. Long-term corticosteroid medication for non-endocrine disease is the most common cause of secondary hypoadrenalism. The hypothalamic-pituitary axis and the adrenal may both be suppressed and the patient may have vague symptoms of feeling unwell. Thus, 17-hydroxyprogesterone, androstenedione and testosterone levels are increased, leading to virilization. The other forms affect 11-hydroxylase, 17-hydroxylase, 3-hydroxysteroid dehydrogenase and a cholesterol sidechain cleavage enzyme (p450scc). Adequacy of glucocorticoid dose is judged by: Clinical wellbeing and restoration of normal, but not excessive, weight Normal cortisol levels during the day while on replacement hydrocortisone (cortisol levels cannot be used for synthetic steroids). In the female, clitoral hypertrophy, urogenital abnormalities and labioscrotal fusion are common, but the syndrome may be unrecognized in the male. Precocious puberty with hirsutism is a later presentation, whereas rare, milder cases only present in adult life, usually accompanied by primary amenorrhoea. Patientadvice All patients requiring replacement steroids should: Investigations Expert advice is essential in the confirmation and differential diagnosis of 21-hydroxylase deficiency, and with ambiguous genitalia such advice must be sought urgently before any assignment of gender is made.
Syndromes
- You will usually be asked not to drink or eat anything for 6 - 12 hours before the surgery.
- Vomiting may occur after every feeding or only after some feedings
- Bladder changes caused by benign prostatic hypertrophy (BPH)
- Stroke
- Infection (a slight risk any time the skin is broken)
- Swollen legs or abdomen (rare in children)
The observed specific activity of hemoglobin protoporphyrin is less than that predicted from the continued availability of labeled glycine for hemoglobin synthesis as determined from the hippuric acid curve treatment uti infection chloromycetin 500 mg overnight delivery. Accordingly symptoms zoloft buy 500 mg chloromycetin otc, they behave as more polar molecules, with rapid (direct) diazoreactivity, and can be excreted in bile without conjugation [4345]. Finally, under certain conditions in vitro, the two nonidentical halves of the bilirubin molecule can dissociate and then reassemble at random [42]. They are, therefore, relatively nonpolar, react slowly with diazo-reagents, and require conjugation as a prerequisite to biliary excretion [4648]. However, only the (4Z,15E) and (4E,15E) photoisomers, which are formed and readily excreted without conjugation during phototherapy of neonatal jaundice [34,35,44,45], are of clinical significance. As an otherwise insoluble molecule, bilirubin formed in the periphery is transported to the liver tightly bound to albumin, at concentrations that far exceed its solubility in protein-free aqueous solutions [50,51]. Adult human albumin has one high-affinity binding site for bilirubin and at least one class of lower affinity sites. Experimental measurements of the affinity of bilirubin for albumin have varied considerably with the methods employed [50], but estimates of a Kd for the high-affinity site have been in the micromolar range by several different approaches [50,52,53]. The determination of these estimates has been based on the assumption that the affinity of bilirubin for albumin is constant, and is independent of the albumin concentration. Under this assumption, until the bilirubin: albumin molar ratio in the circulation exceeds 1: 1, virtually all of the bilirubin present would be bound to the high-affinity site on albumin, and the unbound bilirubin concentration would remain extremely small. This small, unbound bilirubin concentration [54] is, nevertheless, considered to be an important driving force for hepatocellular bilirubin uptake (see later). Under this model, if the 1: 1 molar ratio of bilirubin to albumin is exceeded, the unbound bilirubin concentration increases rapidly with further increases in total bilirubin. In the neonatal period, increased levels of unbound bilirubin can cross the bloodbrain barrier, leading to the serious neurological consequences of kernicterus [5558]. Similar neurotoxicity may, rarely, occur in adolescents and adults who develop sufficiently high concentrations of unconjugated bilirubin to exceed the critical 1: 1 bilirubin: albumin molar ratio [59]. This is, in fact, the only clinically significant potential toxicity of hyperbilirubinemia. Since a normal albumin concentration is 4 g/dL (600 mol/L), and a 1 mg/dL bilirubin concentration represents 17. The oxygen functions on the A and D rings are depicted as the lactam tautomers, and the bridge carbons at positions 5 and 15 are shown in the Z configuration. In this configuration they and their attached hydrogens project toward the substituted positions on the adjacent pyrrole rings, just as in the protoporphyrin ring from which bilirubin is derived. Rings A and B lie in one plane, and C and D lie in another, with the interplanar angle being approximately 98.
Specifications/Details
Common Nightshade (Bittersweet Nightshade). Chloromycetin.
- How does Bittersweet Nightshade work?
- Acne, itchy skin, boils, broken skin, warts, arthritis-like pain, nail bed swelling, eczema, promoting water loss (diuretic), pain relief, and calming nervous excitement.
- Are there safety concerns?
- Dosing considerations for Bittersweet Nightshade.
- What is Bittersweet Nightshade?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96584
Matsuo S medicine nobel prize buy discount chloromycetin 500 mg, Yamane T treatment jokes generic chloromycetin 500 mg visa, Tokuda M, et al: Prospective randomized comparison of a steerable versus a non-steerable sheath for typical atrial flutter ablation. Tada H, Oral H, Sticherling C, et al: Electrogram polarity and cavotricuspid isthmus block during ablation of typical atrial flutter. Yamada T, Murakami Y, Yoshida Y, et al: Electrophysiologic and electrocardiographic characteristics and radiofrequency catheter ablation of focal atrial tachycardia originating from the left atrial appendage. Kottkamp H, Hindricks G, Breithardt G, et al: Three-dimensional electromagnetic catheter technology: Electroanatomical mapping of the right atrium and ablation of ectopic atrial tachycardia. Bastani H, Insulander P, Schwieler J, et al: Safety and efficacy of cryoablation of atrial tachycardia with high risk of ablation-related injuries. Cappato R, Schluter M, Mont L, et al: Anatomic, electrical, and mechanical factors affecting bipolar endocardial electrograms. A consensus statement from the cardiac nomenclature study group, working group of arrhythmias, european society of cardiology, and the task force on cardiac nomenclature from naspe. Gaita F, Haissaguerre M, Giustetto C, et al: Safety and efficacy of cryoablation of accessory pathways adjacent to the normal conduction system. Soejima K, Mitamura H, Miyazaki T, et al: Catheter ablation of accessory atrioventricular connection between right atrial appendage to right ventricle: A case report. Pappone C, Vicedomini G, Manguso F, et al: Risk of malignant arrhythmias in initially symptomatic 30. Catheter Ablation for Ventricular Tachycardia in Patients With Structural Heart Disease William G. The optimal ablation approach and its efficacy are determined by the characteristics of the arrhythmia and the anatomy and location of the arrhythmia substrate, which can often be anticipated from the electrocardiographic characteristics of the arrhythmia and any underlying heart disease. It is important to consider fluid balance, electrolyte abnormalities, anemia, and metabolic abnormalities, such as hyperthyroidism, that might contribute to hemodynamic deterioration or development of uncontrollable arrhythmias during the procedure. The use of external irrigation ablation catheters administers intravascular volume that requires attention to fluid balance and diuresis to avoid development of pulmonary edema or aggravation of heart failure if extensive ablation is needed. If laminated thrombus is suspected, a period anticoagulation therapy with warfarin may be considered with the hope of stabilizing potentially friable thrombus, although the efficacy of this approach is not known. After ablation, continued anticoagulation with aspirin or warfarin is recommended depending on the extent of ablation performed. Drug withdrawal is not always feasible or necessary in patients with frequent episodes and can precipitate electrical storm in some patients. The closer an exit is to a precordial lead, the more negative the S wave in that lead, providing an indication of exit location between the base and apex.
Related Products
Usage: q.3h.
Therefore medications 8 rights chloromycetin 500 mg buy online, these substages had been designated as stage 1 and 2 for patients without and with varices medicine effects best chloromycetin 500 mg, respectively [60]. Even though the study Stages of cirrhosis/portal hypertension the management of varices and variceal hemorrhage should be taken in the context of the different prognostic stages of cirrhosis. This is important because these stages differ not only regarding the prognosis of the patient but also in their predominant pathophysiological mechanisms. Therefore, management strategies individualized at each of the prognostic stages are warranted. Numerous prognostic studies over the years have demonstrated that cirrhosis is not a single entity. In a systematic review evaluating 116 such studies, the median survival of patients with cirrhosis had a very wide range of 1186 months [60], indicating that cirrhosis is a heterogeneous disease. This cutoff also identifies patients with compensated cirrhosis more likely to develop hepatocellular carcinoma [68] and more likely to decompensate after surgical liver resection [69]. As for other substages of cirrhosis, this stratification is not only of prognostic significance but also of pathophysiological/therapeutic significance. In this substage of mild portal hypertension the main mechanism is increased intrahepatic resistance. Of the decompensating events, overt ascites is clearly the most common, accounting for 6080% of initial clinical events, followed by gastrointestinal hemorrhage, while encephalopathy and jaundice occur as the first clinical event in only a minority of patients [61,71]. Although the main pathogenic mechanism in compensated cirrhosis is portal hypertension, in decompensated cirrhosis the main pathogenic mechanism is the hyperdynamic circulatory state and liver insufficiency, although portal hypertension remains prognostically significant [72], particularly in patients with variceal hemorrhage [73,74]. Substages in the setting of decompensated cirrhosis are not yet as clearly defined as in the compensated stage. It is now clear, however, that the different decompensating events have in themselves a different prognosis. Previously, patients with decompensated cirrhosis had been stratified into those with ascites with or without varices (stage 3) and those with gastrointestinal bleeding with or without ascites (stage 4) [75], with a poorer prognosis for stage 4. However, this substaging needs to be abandoned as it has been shown that patients with ascites have a significantly poorer outcome than those presenting with variceal hemorrhage as the only decompensating event [64], including a study that used competing risk analysis [61]. This has led to a restaging of cirrhosis, based on 5-year mortality rates, in which patients with gastrointestinal bleeding as sole decompensating event, those presenting with a nonbleeding complication (mainly ascites) as sole decompensating event, and those with two or more concomitant have progressively worse prognoses (20%, 30%, and 88%, respectively) [61]. The natural history of cirrhosis consists of a progression across different prognostic stages, with the compensated and decompensated stages being the most important. A stage of "further" decompensation, as defined by the development of refractory ascites, hepatorenal syndrome, recurrent variceal hemorrhage and recurrent/persistent hepatic encephalopathy, is likely to provide a larger prognostic differential among these patients. A final stage characterized by multiorgan failure, termed "acute-on-chronic" liver failure, is associated with the worst prognosis.
Additional information:
10 of 10
Votes: 28 votes
Total customer reviews: 28
Tags: 500 mg chloromycetin buy fast delivery, chloromycetin 250 mg purchase on-line, generic chloromycetin 500 mg buy on line, cheap chloromycetin 500 mg visa, chloromycetin 250 mg without a prescription, purchase chloromycetin 500 mg otc, chloromycetin 500 mg visa, buy 250 mg chloromycetin with amex
Customer Reviews
Hamid, 29 years: The cause is multifactorial, with contributions from direct medication nephrotoxicity.
Kadok, 43 years: Glibenclamide Glipizide and Glimepiride Gliclazide Chlorpropamide Biguanide (metformin) Metformin is the only biguanide currently in use, and remains the best validated primary treatment for type 2 diabetes.
Mojok, 35 years: Nevertheless, patients may die of fulminant hepatitis with only a modest elevation in serum bilirubin level.
Sebastian, 58 years: Several reports have linked acute BuddChiari syndrome during pregnancy with an underlying procoagulant state, such as primary antiphospholipid [127], factor V Leiden mutation [128], thrombotic thrombocytopenic purpura [129], or myeloproliferative disease [130].
Vibald, 23 years: Very infectious and/or readily disseminated organisms: high mortality with a major impact on public health B.
Esiel, 24 years: There are certain populations, such as those with enlarged atria, for which the CoxMaze procedure has unacceptably high postoperative failure rates.
Ernesto, 21 years: Although lifelong immunosuppression is often required postoperatively, the procedure usually provides symptomatic relief and correction of the phenotype in types 2 and 3 disease.